


Last Updated: December 30, 2017
Anadrol History and Overview:
Anadrol is known (sometimes notoriously) as being one of the contenders for being the strongest oral anabolic steroid commercially available. It closely competes with Dianabol (Methandrostenolone), and steroid-using bodybuilding circles have always debated which of the two are stronger. Anadrol is the brand and trade name for the anabolic steroid more formally known as Oxymetholone. This is not to be confused with Oxandrolone, which is otherwise known as Anavar. Oxymetholone is Anadrol. Anadrol’s details were first released in 1959[1]. Almost immediately after, the pharmaceutical company Syntex sold Oxymetholone under the name Anadrol-50 while Parke Davis & Co. also manufactured it, though they did so under the Androyd trade name. After its initial release onto prescription markets, Anadrol was quickly prescribed and used for a multitude of medical conditions ranging from geriatric atrophy to combating infections. It’s most noted and popular use as a medication, however, was in the treatment of anemia. Anadrol was prescribed here to increase the red blood cell count and hemoglobin levels of the anemic individual.
This was because of Anadrol’s ability to stimulate erythropoiesis at a very high rate. Although all anabolic steroids exhibit this capability, Anadrol’s ability to stimulate erythropoiesis far exceeds that of any other anabolic steroid. In these cases, Anadrol has been shown in studies to increase red blood cell production by a factor of 5 fold[2]. As far as its general effectiveness as an anabolic steroid for muscle-building purposes is concerned, studies have demonstrated that it has exerted notable anabolic effects on muscle-wasting AIDS patients, causing them to actually gain 8kg of weight while those who were administered a placebo not only lost weight but also experienced an increase in mortality[3]. It is for this reason that Anadrol tends to be prescribed almost primarily in this day and age for AIDS patients and muscle wasting diseases.
Chemical Characteristics of Anadrol:
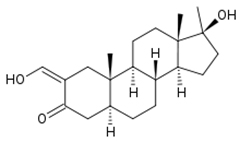
Anadrol is derived from Dihydrotestosterone (DHT), belonging to the family of Dihydrotestosterone (DHT) derived anabolic steroids. This means that Anadrol is basically Dihydrotestosterone modified. Other compounds belonging to this ‘DHT family’ of anabolic steroids include Winstrol, Primobolan, Masteron, Anavar, as well as several others which are all derivatives of the parent anabolic steroid DHT. The common factor in all of these DHT-derivative analogues is that, in one way or another, they are all modified forms of DHT and thus DHT could be considered the ‘parent’ or ‘progenitor’ hormone of these anabolic steroids. Anadrol differs from its parent hormone DHT by the addition of a methyl group attached to it, as well as a 2-hydroxymethylene group attached to a carbon in the first cycloalkane ring of the steroid structure. These modifications allow Anadrol to remain active in muscle tissue, which is where Dihydrotestosterone would normally be rendered inactive by its reduction to other metabolites once it enters muscle tissue. The enzyme responsible for doing this to Dihydrotestosterone, which is present in large amounts in muscle tissue, is 3-hydroxysteroid dehydrogenase. With the chemical modifications mentioned, this enzyme does not interact with Anadrol. This allows Anadrol to be heavily active in muscle tissue, and lends to its very strong potency. Anadrol possesses an anabolic rating of 320 (a little more than 3 times the strength of Testosterone, with its anabolic rating of 100). It has also been determined that Anadrol also possesses reduced androgenic strength compared to that of Testosterone, where Anadrol holds an androgenic rating of 45 (compared to Testosterone’s androgenic rating of 100).

Advertisement
One of the unique and mysterious characteristics possessed by Anadrol is that although it is a derivative of DHT, it possesses a very high level of Estrogenic activity. It is typically known that DHT-derivative anabolic steroids should be unable to convert into Estrogen via the aromatase enzyme and therefore elicit no Estrogenic effects, but this is very different with Anadrol. Anadrol is well known for causing water retention, bloating, gynecomastia, and other Estrogenic effects on the body even though it does not convert into Estrogen. It is believed that Anadrol itself acts as an estrogen in certain tissues. This will be further expanded upon and discussed later on, but it is imperative for any potential user to understand that first and foremost that although Anadrol is a DHT-derivative, one will not experience the lean hard gains typically seen with DHT-derivatives. Anadrol is notorious for its Estrogenic effects that cannot be combated with aromatase inhibitors due to its inability to convert into Estrogen.
Anadrol is an orally active anabolic steroid, which means it has been C17 Alpha Alkylated in order to allow the anabolic steroid to make the first pass through the liver without suffering destruction through liver metabolism. Anadrol, however, is very well known for its very harsh hepatotoxicity, which will be explained in greater detail shortly. Anadrol’s chemical modifications and chemical structure (including its C17 Alpha Alkylation) makes it very resistant to hepatic breakdown (liver metabolism). The greater resistance a substance has to hepatic breakdown, the more toxicity and strain on the liver will be experienced – and Anadrol is notorious for its liver toxicity, and is perhaps regarded as the most liver toxic oral anabolic steroid conventionally available.
Anadrol Side Effects:
Anadrol is an orally active C-17 alpha alkylated anabolic steroid, and as such, it exhibits hepatotoxicity and negative effects where the liver is concerned. Anadrol is, in fact, the worst offender for this among all commercially available anabolic steroids. It is likely very possible that this has been over-exaggerated among the bodybuilding community, but it should nevertheless be taken very seriously. Interestingly enough, Anadrol possesses a chemical modification that is actually supposed to reduce hepatotoxicity[4]. The reality, however, is that Anadrol still raises liver enzyme markers during use as demonstrated in studies with HIV and AIDS patients[5] [6]. It is therefore highly advised to limit Adrol to cycle lengths of no greater than 4 – 6 weeks of use, and to supplement with plenty of proven liver support compounds.
Things become stranger with Anadrol when other side effects are investigated. It is well-known that Anadrol is a DHT (Dihydroteststerone) derivative, and therefore does not convert into Estrogen. However, Estrogenic side effects are known to be notoriously prominent with Anadrol, producing side effects such as bloating and water retention (often reported as extreme) with concomitant increases in blood pressure, and the development of gynecomastia. The use of a SERM (such as Nolvadex) will mitigate gynecomastia, but will not solve water retention (and resultant blood pressure) issues. Aromatase inhibitors will not work with Anadrol, as it has no interaction with the aromatase enzyme to begin with. Although it is speculated that Anadrol may act as a Progestin causing these side effects, studies have demonstrated that Anadrol does not hold any Progestogenic properties[7]. The most likely (though yet unconfirmed) explanation would be that Anadrol may possibly interact with the Estrogen receptor directly, or that a metabolite of Anadrol might possibly do this as well.
The evidence of strange metabolites of Anadrol becomes even stronger when other Anadrol side effects are investigated. For example, in terms of androgenic side effects, they tend to be fairly reduced in comparison with Testosterone. However, Anadrol does not convert into DHT and instead is metabolized into 17-alpha-methyl dihydrotestosterone (Mestanolone)[8]. Mestanolone is a stronger androgen, and therefore some degree of androgenic side effects can be expected from Anadrol (such as oily skin, acne, male pattern baldness, benign prostatic hyperplasia, etc.).
Lastly, as with all oral anabolic steroids, Anadrol tends to impact the cardiovascular system negatively in an extreme manner, producing vast alterations in blood cholesterol profiles (for both LDL and HDL)[9].
Anadrol Cycles and Uses:
Cycles including Oxymetholone are normally of the type that are intended for bulking, strength-gaining, and general overall mass. Anadrol cycles are poorly suited for the purpose of cutting, fat loss, pre-contest, or anything of the like. Although Anadrol can indeed be used to aid and accelerate in fat loss, it is a poor choice because of its Estrogenic effects, notably water-retention and bloating. This side effect serves to provide the physique with an overall soft and smooth look to it, which blurs, obscures definition, making it difficult to visually gauge fat loss. This is made worse by the fact that Anadrol does not convert into Estrogen, and therefore imposes this effect on the user by some as-of-yet-unidentified other means. Therefore, and aromatase inhibitor in this case would not work to reduce the bloating effect.
Anadrol cycles are normally composed of Anadrol as a kickstarting compound for the first 4 – 6 weeks where it is supplementary to other injectable base compounds that are used for similar purposes, such as Testosterone Enanthate, Deca-Durabolin (Nandrolone Decanoate), Trenbolone Enanthate, etc. It can also be utilized in the middle of a cycle in order to push through any sticking points or plateaus in training progress. Additionally, some users throw it into the end of a cycle in order to boost the end of a cycle and act as a ‘finisher’ compound in a cycle, leaving the user to end off their cycle with some very impressive strength and size gains as they move into the PCT (Post Cycle Therapy) phase.
Anadrol cycles should not extend beyond 4 – 6 weeks due to hepatotoxicity issues. However, other compounds used with it, such as injectables, can be utilized beyond Anadrol’s ending period.
Anadrol Dosages and Administration:
Prescription guidelines for Anadrol varied a great deal throughout the 1950s – 1980s and was dependent on the medical condition treated, as well as constantly changing FDA guidelines. Medical Anadrol dosages ranged from 2.5mg taken three times per day all the way up to 30mg per day. Eventually in the 1970s, the FDA issued a guideline of 1 – 2mg per kg of bodyweight per day.
Because Anadrol is most commonly manufactured in 50mg tablets, bodybuilding and athletic purposes call for 25 – 50mg per day for a beginner. Intermediate users are known for using a range of 50 – 100mg per day, and although approaching risky limits, advanced users as high as 150mg per day. Generally, however, most users whether beginner, intermediate, or advanced, should seldom require more than 50mg per day due to the sheer potency and strength of Anadrol as an anabolic steroid. This is especially the case when studies have demonstrated that a 100mg Anadrol dosage is indeed more effective than a 50mg Anadrol dosage, but beyond 100mg the results will be no more effective than 100mg itself, and diminishing returns begin to manifest[10].
An additional point of interest about Anadrol dosages is that many users report a reduction in appetite directly proportional to the dose utilized, and studies have shown that it also increases glucose intolerance and insulin resistance[11], thus making nutrient use by the body less efficient.

ANDROLIC Britsh Dispensary 50mg Tabs
Anadrol dosages can and should ideally be split throughout the day so as to ensure stable and steady blood plasma levels of the hormone. Anadrol exhibits a half-life of about 8 to 9 hours in the body, and therefore a schedule involving a morning (AM) dose followed by an afternoon/evening (PM) dose is best.
How to Buy Anadrol:
Anadrol is a pretty common and fairly popular anabolic steroid on the market, and is one that is sure to be manufactured, stocked, and supplied by most, if not all major sources and vendors. As with any anabolic steroid, Anadrol can be purchased as either a pharmaceutical grade or underground lab (UGL) grade anabolic steroid product. Differences in quality, and especially in price, exist between the two. Generally, however, Oxymetholone is a fairly affordable and decently priced anabolic steroid on the market, especially when compared with those compounds that are rarer and more exotic.
Pharmaceutical grade Adrol can run for around $1.30 – $2.50 per 50mg tablet. Underground quality Anadrol can often be found and bought for $0.75 – $2.30 per tablet. Of course, this is a very large range and is very dependent on not just the grade of product (pharma vs. UGL), but also on the actual type of source utilized, with the two major types being internet and in-person ‘dealers’. There are other differences and factors that affect price as well, such as minimum order limits and whether or not the source may be intentionally taking advantage of less experienced anabolic steroid users and beginners that may not know better (this is common among the in-person dealers).
Latest Research:
December 30, 2017: At the University of Southern California sports scientists examined the results of placebo, 50mg and 100mg per day given to elderly healthy patients. The then published the results of the study in 2003 showing the positive effects Oxymetholone has on muscle growth and fat loss.
The study showed that the men that had taken the compound saw an increase in lean body mass by approximately 3.3 kg, and when it comes to the men who took the bigger 100mg dose, they had actually gained over 4.2 kg. The fat mass in both of the groups actually went down by 2.6 and 2.5 kg, thereby showing that it could not only produce lean body mass but it could eliminate fat as well. When they actually did scans of their bodies, they found that the 50 mg men has lost almost 2 kg of fat mass in their trunk, which is the torso area. And those that had taken the double dose at 100mg lost about 2.2kg. Based on the results of the study, it appears that most of it was lost in their midsection and torso. This is often where males primarily tend to store fat mass.
The study also showed a number of negative effects, mostly hepatoxicity (liver damage) and a reduction in HDL (good cholesterol). This is why its often suggested that Anadrol use should not excessed 4-6 weeks of continues usage.
Source: https://www.ncbi.nlm.nih.gov/pubmed/12388137
Anadrol Information:
 Oxymetholone (AKA Anadrol, Anadrol-50)
Oxymetholone (AKA Anadrol, Anadrol-50)
Chemical Name: 17β-hydroxy-2-hydroxymethylene-17-methyl-5α-androstan-3-one
Molecular Weight: 332.48 g/mol
Formula: C21H32O3
Original Manufacturer: Syntex
Half Life: 8 – 9 hours
Detection Time: 2 months
Anabolic Rating: 320
Androgenic Rating: 45
Anadrol References:
- 2-Methyl and 2-hydroxymethylene-androstane derivatives. Ringold HJ et al. J am Chem Soc 1959;81:427-32.
- Oxymetholone treatment for the anemia of bone marrow failure. Alexanian R, Nadell J, et al. Blood. 1972;40:353-6.
- Schroeder et al. Am J Physiol Endocrinol Metab 284:E 120-28
- Effects of various 17 alpha alkyl substitutions and structural modifications of steroids on sulfobromophthalein (BSP) retention in rabbits. Lennon HD et al. Steroids 7 (1966): 157-70.
- Long-term oxymetholone use in HIV patients not associated with significant hepatotoxicity. Hengge UR et al. Poster presented at the Third International Conference on Nutrition and HIV Injection; April 22-25, 1999; Cannex, France.
- 1984 Jun;114(6):2100-6.
- Les hormones anabolisantes du point de vue experimental. P.A. Desaulles. Helv. Med. Acta 1960;479-503.
- Studies on anabolic steroids-8. GC/MS characterization of unusual seco acidic metabolites of oxymetholone in human urine. J Steroid Biochem Mol Bio 42 (1992):229-42.
- Effects of an oral androgen on muscle and metabolism in older, community-dwelling men. Schroder et al. Am J Physiol Endocrinol. Metab. 284:E 120-28.
- J Clin Endocrinol Metab. 1981 Nov;53(5):905-8. Epilepsy Behav. 2004 Apr