


Introduction
The potential side effects associated with anabolic steroid use is a very prominent topic amongst not only athletes and bodybuilders, but also among individuals that do not hold any involvement what so ever in athletics or fitness. Most usually, the first question an individual will have when confronted with the topic of anabolic steroids is: “what are the steroids side effects?” and associated questions within this topic of steroids side effects, such as: long term and short term side effects, male and female specific side effects, and many others. It is a very rich, dense, and vast topic that could be discussed for days on end.
This particular article will deviate from the typical scare tactics so very common of the mass media and governments, and instead focus on the proper context under which anabolic steroids side effects should be viewed upon: how these side effects occur, under what conditions, in which circumstances, how they can be dealt with, what can be done about them, and how prominent are the various side effects?
The sensationalist and biased mass media would have us believe that anabolic steroids are extremely high-risk drugs that are the cause of acute death as well as long-term death. This could not be farther from the truth, as the medical establishment regards anabolic steroids as low-risk therapeutic compounds with a high degree of safety. Regardless, anabolic steroids can and do present various side effects, but these side effects must be viewed upon in the proper context rather than the extreme sensationalist and biased manner that the mass media and governments utilize in order to scare the population away from these substances.
When it comes to the issue of context, a perfect example is real world data in the form of clinical studies that have demonstrated that the frequency of side effects experienced by anabolic steroid users was that of 96.4%[1]. To an individual unaware of proper contextualization of situations and data, he or she may react shockingly to this statistic and conclude that anabolic steroids are indeed a high-risk drug where the rate of experiencing side effects are close to 100%. The truth is that the figure of 96.4% as determined by the clinical study referenced refers to a rate of experiencing steroids side effects at 96.4% across the board. The percentage given is a much generalized figure, and does not specify as to what percentage of that figure are severe side effects, minor side effects, and/or how many individuals simply experienced an extremely minor side effect such as a tiny increase in acne formation from week to week. Such a side effect is hardly regarded as ‘high-risk’ or life-threatening, and the fact of the matter is that the majority of side effects experienced, if experienced at all, from anabolic steroid use are merely minor, reversible, and cosmetic side effects. It is very evident that the statistical data in regards to the side effects associated with anabolic steroids is often misinterpreted and taken out of context. One must always keep this in mind in regards to such a topic that is so vast, diverse, and dynamic.
It is first very important to remind the reader not to paint an image of anabolic steroids side effects with a single large brush. This means that blanket statements must not be made concerning side effects and how they affect individuals. The dynamic of steroids side effects is so complex and diverse that every effort must be taken to clarify the common rumors, misconceptions and blanket generalized statements in regards to the side effects of anabolic steroid use.
Side effects resultant from anabolic steroid use can be split into three distinct and different categories:
1. General side effects
2. Male-specific side effects
3. Female-specific side effects
Furthermore, only the most common anabolic steroids side effects that are shared among all anabolic steroids will be covered in this article. There also exist a small number of anabolic steroids that possess side effects unique to them that are not shared with most other anabolic steroids – these will not be covered here. It must be first understood that anabolic steroids are hormones that affect and control several different functions and aspects of the human body and that its effects are very diverse.
The Four Laws of Side Effects
Before delving into the different side effects, the following points must be made clear to the reader:
– Not every individual will experience all side effects associated with anabolic steroid use.
– Some individuals will experience certain side effects and not experience various others.
– Some individuals will not experience any side effects at all.
– Side effect intensity/severity will vary and differ between individuals.
– Side effects are dependent on many different factors and do not affect every individual in the same manner.
– Side effects should always be referred to as potential side effects for these reasons.
Therefore, four laws (or rules) of steroids side effects have been developed in order to explain how and why side effects affect various individuals differently, and they are ranked in order of importance/influence (greatest to lowest from 1 – 4):
1. Genetics – Every single individual will respond in a different manner to any chemical, compound, anabolic steroid, food or drug in existence. Because one person may experience a particular side effect or various side effects, it does not mean that another individual will experience the exact same thing. Each person is governed by a blueprint or a list of rules as to how he or she will respond to almost anything, and these blueprints are known as genetics, or DNA. Various genetic responses to certain stimuli, food, drugs, or even general experiences can and do also change over time.
2. Dose and duration – Increased doses most usually result in increased incidences and severity of side effects. It is very possible for certain individuals to possess a higher tolerance to various compounds and would be able to, for example, run ridiculously high doses of 2,000mg weekly of an anabolic steroid and experience no ill side effects, while other individuals may run 300mg weekly of the same anabolic steroid and find they possess a high sensitivity and experience a plethora of different side effects such as gynecomastia, bloating, acne, etc. Duration is also a very influential factor, as it need not be explained that the longer a particular anabolic steroid is utilized, the increased incidence of side effects will also present themselves as the duration of use becomes longer and longer.
3. Age – Related to genetic response changing over time, age is a very important factor as to whether or not an individual will experience a side effect and how severe it will be. For example, various individuals may be able to run aromatizable anabolic steroid cycles with no aromatase inhibitor or Estrogen blocker and experience no gynecomastia symptoms. 15 years later, this same individual may run a similar cycle and suddenly experience gynecomastia development. This is indicative that the person’s body has changed with age and is now reacting in a very different manner to the effects of anabolic steroids.
4. Type of anabolic steroid or compound used – There exist hundreds of different anabolic steroid analogues and compounds for the purpose of performance and physique enhancement. Many of them possess different attributes, capabilities, and properties (some distinctly so more than others) and therefore different side effects can result with varying intensities.
General Steroids Side Effects
Anabolic steroids, as previously mentioned in the introductory section of this article, anabolic steroids are hormones that are either Testosterone itself, or analogues/derivatives of Testosterone. These are important hormones essential for proper healthy function of the human body, and they govern, affect, and control a myriad of different functions and aspects of the human body. Therefore, the effects of anabolic steroids on the body (both undesirable and desirable effects) are very diverse and quite dynamic. These hormonal effects are so dynamic in nature that it is considered a very poor demonstration of intelligence to relegate the effects and side effects of anabolic steroids to simplistic views in which an individual generalizes steroids side effects, and generalizes such a topic.
What will be covered here are the most prominent general steroids side effects. This refers to the potential side effects that are not gender-specific and can and will affect all genders of all age groups equally.
Cardiovascular Side Effects (General)
When anabolic steroids are utilized at the doses required for physique and performance enhancement (also referred to as bodybuilding doses), all anabolic steroids can and do have negative effects on the cardiovascular system of the human body. The degree and severity by which these negative cardiovascular changes occur is dependent on which anabolic steroid is used (some exhibit more of a negative effect while others do not, and some even exhibit improvements), dose, duration of use, personal response, and age. Many of these negative cardiovascular effects can be offset with proper nutritional adjustments. It is important to know that even therapeutic doses of anabolic steroids far less than bodybuilding doses are also known to sometimes (and under certain conditions) cause negative cardiovascular effects, though this is far less prominent and frequent. The fact of the matter is that the majority of cardiovascular effects resultant of anabolic steroid use is short-term and reversible. Heart attacks and strokes as a result of solitary anabolic steroid cycles are extremely rare. However, excessive abuse of these drugs in both high doses as well as excessively long cycles and periods of use can contribute to a long-term accumulative effect where an increased risk in the long-term is a possibility.
These cardiovascular steroids side effects include: negative changes in cholesterol levels, ventricular hypertrophy, and blood pressure increases.
Cardiovascular Side Effects (Cholesterol)
All anabolic steroids exhibit negative cholesterol profile changes in the body to varying extent (some exhibit this more and some less). These changes involve the reduction of HDL (the good cholesterol) and increases of LDL (the bad cholesterol). The result of such changes involves an increased risk of arteriosclerosis, and the degree to which these changes occur for the worse are usually dose-dependent (with higher doses increasing the negative changes and the risks). Other factors that affect these negative cholesterol changes are: duration of use, and route of administration. This is where oral anabolic steroids hold a negative reputation for exhibiting a far worse negative impact on cholesterol in comparison to injectable anabolic steroids. This is because the liver serves to function as the cholesterol processing center for the human body, and the increased hepatotoxicity associated with anabolic steroids will result in even worse negative cholesterol changes.
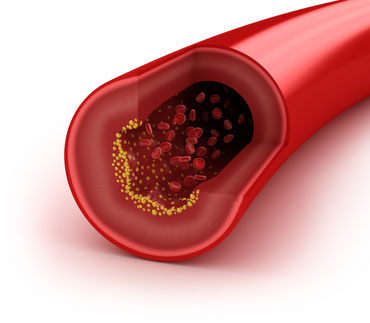 The manner by which these changes occur involves the effect of androgens on hepatic lipase. Hepatic lipase is an enzyme located in the liver which is responsible for the breakdown of HDL (good) cholesterol[2]. It then stands to reason that a reduction in hepatic lipase would result in lower HDL cholesterol levels as this enzyme works to reduce blood plasma levels of HDL cholesterol. Logic might then indicate that as the doses of anabolic steroids increase, this effect too increases in relation to dose. However, this is wrong! One study in which Testosterone Cypionate was administered to test subjects at a dose of 300mg weekly, which resulted in a 25% decrease in HDL cholesterol[3]. However, when the dose in the same study was increased to 600mg weekly, there were no additional reductions in HDL cholesterol, which would indicate that there seems to be a ceiling limiting how much hepatic lipase enzyme activity can be stimulated by anabolic steroids.
The manner by which these changes occur involves the effect of androgens on hepatic lipase. Hepatic lipase is an enzyme located in the liver which is responsible for the breakdown of HDL (good) cholesterol[2]. It then stands to reason that a reduction in hepatic lipase would result in lower HDL cholesterol levels as this enzyme works to reduce blood plasma levels of HDL cholesterol. Logic might then indicate that as the doses of anabolic steroids increase, this effect too increases in relation to dose. However, this is wrong! One study in which Testosterone Cypionate was administered to test subjects at a dose of 300mg weekly, which resulted in a 25% decrease in HDL cholesterol[3]. However, when the dose in the same study was increased to 600mg weekly, there were no additional reductions in HDL cholesterol, which would indicate that there seems to be a ceiling limiting how much hepatic lipase enzyme activity can be stimulated by anabolic steroids.
At the same time, various other anabolic steroid analogues have been found to exhibit far greater negative cholesterol changes even at lower doses, and it has been previously mentioned that oral anabolic steroids that are C17-alpha alkylated tend to exhibit a far greater effect on the negative changes associated with cholesterol. C17-alpha alkylation (also known as methylation) is a chemical modification required to allow an anabolic steroid to become resistant to hepatic metabolism in order to allow high bioavailability of the anabolic steroid through oral administration. This chemical modification also results in increased hepatic strain. One particular study compared the effects of oral Stanozolol (Winstrol) to Testosterone on cholesterol profiles, where 200mg weekly of Testosterone was administered in comparison to 6mg per day of oral Stanozolol[4]. The results of this particular study following 6 weeks of administration of these anabolic steroids demonstrated HDL reductions of 33% – 71% with oral Stanozolol use, and HDL cholesterol dropped only 9% in the subjects administered Testosterone. LDL (bad cholesterol) levels were increased by 29% in subjects administered oral Stanozolol, while subjects administered Testosterone only experienced a 16% increase in LDL. The conclusion here is that oral steroids are far more strenuous to the cardiovascular system in this case than injectable non C17-alpha alkylated compounds.
Estrogen itself is actually known to have positive effects on cholesterol profiles, improving HDL levels and reducing LDL as well. The issue of concern here is the use of ancillary compounds known as aromatase inhibitors during anabolic steroid cycles to the extent whereby circulating Estrogen levels are reduced to sub-physiological levels which is not a good thing. Testosterone in particular has demonstrated in one clinical study to have only a mild impact on HDL cholesterol after a 12 week period where 280mg of Testosterone Enanthate was administered weekly. The cholesterol profiles had later changed for the worse when an aromatase inhibitor was included, which resulted in a significant 25% drop in HDL cholesterol[5]. Estrogen levels should always be controlled and maintained as closely as possible to normal physiological levels. This must be remembered by any potential anabolic steroid user in that Estrogen levels must be closely monitored so as to ensure they are not reduced to the point whereby cholesterol profiles are impacted negatively even further.
Proper attention to a clean diet and the inclusion of various healthy cholesterol promoting foods (such as omega-3 fatty acids and fish oils (at least 2 – 4 grams per day) is essential while on a cycle of anabolic steroids in maintaining healthy cholesterol profiles during cycles, which indeed can be done. The cholesterol changes mentioned as a result of anabolic steroid use are always temporary and always return to normal following cessation of a cycle. This is why it is advised that individuals perform anabolic steroid cycles in the range of 8 – 12 weeks with at least 4 months of a break in between each cycle. Such a protocol should effectively eliminate any risks of long-term accumulative changes in the arteries. Continuous use without breaks is most usually the cause of severe long-term buildup of cholesterol resulting in arteriosclerosis (especially if oral anabolic steroids are utilized for extended periods).
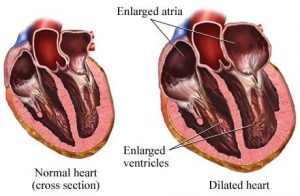
Cardiovascular Side Effects (Heart Enlargement)
Because the human heart is composed of muscle tissue, it too possesses androgen receptors that are available for androgenic anabolic steroids to act on. The fact of the matter is that males naturally manufacture far more Testosterone endogenously than females do, and it has been demonstrated that males on average possess larger hearts than do females[6]. Exercise and intense physical training itself without the use of anabolic steroids is also responsible for the growth of the heart. Types of training also affect the differences in the types of heart enlargement:
 Anaerobic exercise (resistance/weight training): This type of exercise stimulus causes what is known as concentric remodeling, which refers to the thickening of the ventricles (outer wall of the heart) but no growth of the internal wall.
Anaerobic exercise (resistance/weight training): This type of exercise stimulus causes what is known as concentric remodeling, which refers to the thickening of the ventricles (outer wall of the heart) but no growth of the internal wall.
Aerobic exercise (endurance training): This type of exercise stimulus causes what is known as eccentric remodeling, which is characterized by the growth of the internal wall of the heart but no growth of the ventricles (outer walls).
Despite the different variations in heart growth, it is common knowledge that no disruption in actual heart function has ever been observed, indicating that these changes do not affect proper heart function (diastolic function). Furthermore, the heart muscle adapts according to the level of exercise stimulus provided. This means that when training and exercise is halted, the heart will, after a certain period, begin to decrease in size and revert back to a smaller size. This is a typical characteristic of all muscle tissue whereby if the exercise stimulus is halted, muscle atrophy will eventually occur.
Anabolic steroid use in particular does increase the probability for the enlargement (thickening) of both ventricular walls of the heart (left and right ventricles)[7]. However, it is the left ventricle which has been observed in anabolic steroid users to exhibit a larger increase in muscular size[8]. Remember that these same changes are found in steroid-free athletes as well, but it is in anabolic steroid using athletes where the size increases of the heart muscle is observed as being greater than those of steroid-free athletes.
An interesting note in the differences here is that anabolic steroid using athletes who have left ventricle growth beyond a certain point have exhibited impaired heart function and efficiency[9].
The degree to which the heart muscle will experience significant growth changes has been found to be directly related to the doses used, where higher and higher doses of anabolic steroids will often result in greater growth of cardiac tissue. The size of the heart has also been found to shrink or grow depending on the habits of the anabolic steroid user. For example, not only does dose and duration of use determine the size of growth of the heart muscle, but the heart will also shrink in size over time when anabolic steroids are discontinued[10].
In general, the subject of heart growth and whether or not it is actually a benefit to the athlete or a detriment is an ongoing investigation and debate in the field of sports medicine.
Cardiovascular Side Effects (Blood Pressure)
Blood pressure elevations are a possibility of steroids side effects, but this tends to occur only in certain select situations and conditions. First and foremost, blood pressure increases are commonly the result of increased water retention caused by increased Estrogen levels as a result of aromatizable androgens being aromatized into Estrogen by the aromatase enzyme. Water retention and bloating often causes blood pressure increases due to the increased fluid retention both extracellular and intracellular, and imposes increased pressure on the arterial walls. This side effect can effectively be eliminated by either the use of anabolic steroids that do not convert into Estrogen, or through the use of an aromatase inhibitor (compounds such as Aromasin, Arimidex, and Letrozole) that serve to disable the enzyme responsible for the conversion of androgens into Estrogen: aromatase. With a large percentage of these enzymes effectively disabled, Estrogen conversion will grind to a halt and total circulating blood plasma levels of Estrogen in the body will drop, as will the water retention caused by the Estrogen, and subsequently the heightened blood pressure will reduce as well.
The majority of blood pressure elevations in anabolic steroid users have been found to be moderate rather than extreme or severe. There are other factors in addition to the cause of Estrogen and water retention that cause blood pressure increases in anabolic steroid users. However, the primary means of blood pressure increase is that of either excessive Estrogen conversion, or a poor diet that is too rich in sodium and simple carbohydrates. Blood pressure can be maintained and kept well into the normal (or even impressive) range in anabolic steroid users that take care to avoid large Estrogen increases, as well as maintaining a very clean low to moderate sodium content diet without any simple sugars or carbohydrates.
Cardiovascular Side Effects (Polycythemia)
Polycythemia is a condition in which an individual possesses a red blood cell count that is excessively high above the normal range. This is very common in all athletes, especially endurance athletes. Increased physical demands caused by regular training and exercise result in an increased demand for oxygen transport to the muscles. The result is an increase in red blood cell production, as red blood cells are responsible for oxygen transport in the body. Hemoglobin is the protein located in the center of red blood cells, which is the protein that oxygen binds to so that it may be carried by the red blood cell to tissues that require oxygen. Therefore, ‘high hemoglobin’ is the same thing as ‘high red blood cells’. The result of regular intense training is an increase in red blood cells for the purpose of more efficient oxygen transport to cells during exercise, which further translates into a lesser breathing effort required during exercise and physical exertion.
Anabolic steroids increase red blood cells by way of stimulating the kidneys to provide increases of the hormone Erythropoietin (EPO). EPO then travels to bone marrow where it signals the production of red blood cells. The result is an increased hemoglobin/red blood cell count. Polycythemia refers to an excessive overproduction of red blood cells, which can sometimes occur with anabolic steroid use (especially in users that utilize very high doses and/or engage in excessive duration of use). The problem with the increase in red blood cell count is in the ability to generate higher blood pressure and increased viscosity (thickness) of the blood. Circulation of blood can become impaired if the viscosity of it becomes excessive. The average hemoglobin level for an individual is known to be in the range of 40.7% – 50.3% in males, and 36.1% – 44.3% in females (these are all considered non-athletes). Bodybuilders and athletes that do not use anabolic steroids are known to hold an average hemoglobin level of 45.6%. Anabolic steroid users were determined in one study to hold an average hemoglobin level of 55.7%[11].
High hemoglobin levels, if not rising beyond a certain level, should not pose too much of a risk. In addition, the average life span of a red blood cell is that of 120 days (4 months), and so it therefore stands to reason that if anabolic steroid cycles are kept within reasonable lengths and considerable break time in between cycles is provided, then polycythemia should not present itself as a large risk factor. It is always important for every anabolic steroid user to engage in regular blood testing so as to monitor these factors, and if hemoglobin levels have risen beyond a certain point that administration of any anabolic steroids should be halted immediately followed by a period of non-use so as to allow the body to normalize.
Hepatotoxicity Side Effects
Anabolic steroids in and of themselves are non-toxic to the liver. The hepatotoxicity issue is resultant of the use of oral anabolic steroids, specifically due to the chemical modifications required in order to allow oral bioavailability of the hormone. Anabolic steroids unmodified when ingested orally are metabolized in large amounts by the liver into inactive metabolites to be excreted from the body. This results in insufficient amounts of the anabolic steroid reaching the bloodstream to do its job. For an anabolic steroid to be able to become effective through oral administration, it must be modified at the 17th carbon where a methyl group is bonded to it, known as C17-Alpha Alkylation (also known as methylation). This alkylation grants the anabolic steroid further resistance to hepatic metabolism. The greater resistance a substance has to hepatic breakdown, the more toxicity and strain on the liver will be experienced. This modification, however, allows the anabolic steroid to survive liver metabolism and introduce a high percentage of the anabolic steroid into the bloodstream.
Injectable anabolic steroids that do not possess C17-alpha alkylation do not present any problems where the liver is concerned as evidenced by clinical data. Studies have investigated the potential for hepatotoxicity with Testosterone used at high doses (400mg daily, which equates to 2,800mg weekly) in several male test subjects for a 20 day period where the route of administration was actually oral instead of intramuscular injections. The idea here was to saturate the liver with high amounts of Testosterone (all orally ingested substances make what is known as a ‘first pass’ through the liver and interact with the liver at a far greater rate than the injectable route of administration). The result of the study was that no changes were observed[12]. Therefore, hepatotoxicity is not of any concern where non-methylated injectable anabolic steroids are concerned except in very rare instances most often in which the user possessed an unknown liver problem prior to use.
Liver hepatoxcity from anabolic steroids
As far as C17-alpha alkylated oral anabolic steroids are concerned, liver problems are usually never resultant of proper responsible and judicious use. Excessive use both in dose and duration has demonstrated moderate liver problems to severe and life-threatening liver problems in users in the past. It is also important that every individual ensure they do not possess any underlying liver issues prior to engaging in use of these types of compounds.
Specifically, methylated oral anabolic steroids are protected (by the C17-alpha alkylation) from metabolism in the liver where the enzyme 17beta-hydroxysteroid dehydrogenase will otherwise normally metabolize anabolic steroids (that do not possess C17-alpha alkylation) into inactive forms that do not reach the bloodstream. This enzyme effectively deactivates anabolic steroids that are not methylated for oral use. Although some anabolic steroids will bypass this breakdown, the majority usually succumb to the enzyme 17beta-hydroxysteroid dehydrogenase.
The most common form of hepatotoxicity as a result of excessive oral anabolic steroid use is known as a condition called Cholestasis[13]. This is a condition whereby bile flow in the liver becomes either completely halted or at the very least disrupted. This can result from either a physical blockage, or a chemical one. What occurs here is that the blockage results in a buildup of bile salts and bilirubin in the liver and bloodstream. In large enough quantities, this build-up can become toxic to the hepatic cells of the liver and kill them. The severity of this condition can range from very minor and discomforting to life-threatening. Minor cases are recoverable in a matter of weeks while more severe cases may require months or more of recovery time.
It is therefore recommended to utilize oral C17-alpha alkylated anabolic steroids in a judicious manner for no longer than a 6 – 8 week period (or 4 – 6 weeks in the case of more severely hepatotoxic oral compounds). It is also highly recommended that users supplement with a proven liver support and health supplement, such as TUDCA/UDCA while using oral anabolic steroids[14].
Androgenic Side Effects (Acne)
Androgen receptors exist underneath the skin where androgenic anabolic steroids can bind to these receptors and stimulate an increase in sebum secretion, resulting in oily skin. Anabolic steroids can also increase the size of these glands (known as sebaceous glands)[15]. Excessive sebaceous gland stimulation can result in follicles and pores becoming overloaded with sebum, dead skin, and dirt which results in acne. This is not regarded as a life-threatening side effect and ranges in severity between individuals so much so that some may not experience acne at all, others may experience minor acne, and some will experience severe breakouts. The use of topical anti-androgens such as Nizoral 2% shampoo has proven to be very successful in treating the issue of acne as well as male pattern baldness[16]. Nizoral contains the active ingredient Ketoconazole, which acts as an androgen blocker wherever it is topically applied (to the scalp, or on various areas of the skin where androgen-related acne may occur). Topically, Ketoconazole is an androgen receptor antagonist, competing with androgens such as Testosterone and DHT for androgen receptor binding in the scalp or skin. Ketoconazole serves to block androgens from binding to the receptors on the skin and scalp or wherever it is applied to. The buildup of sebum and/or the resultant acne is usually cleared with the discontinuation of anabolic steroids.
Androgenic Side Effects (Male Pattern Baldness)
Male Pattern Baldness (MPB) is a potential side effect resultant of anabolic steroid use. However, this is a poorly understood condition among the general population, even for MPB that is not caused by anabolic steroid use. Anabolic steroids can bind to androgen receptors located in the scalp and trigger male pattern baldness in individuals that possess the genetic trait required for the condition to manifest itself and can occur in both men as well as women. Note that the genetic sequence for male pattern baldness must be inherited and in possession of the user in order for this side effect to become triggered by androgens. Those who do not possess this genetic trait required will not experience this effect at any dose.
Individuals can elect to either utilize a topical androgen blocker, such as Nizoral 2% (explained above) or through the use of 5-alpha reductase (5AR) inhibitors. 5AR is the enzyme responsible for the conversion of Testosterone into the much more powerful androgen Dihydrotestosterone (DHT). This enzyme is located in various tissues in the body (the prostate, scalp, and skin). It is through the conversion to DHT where the majority of more severe androgenic side effects tend to manifest. Ancillary drugs such as Proscar or Dutasteride (5AR inhibitors) can be utilized to effectively inhibit the 5-alpha reductase enzyme and thereby eliminate DHT at the root of its cause. This will not, however, completely eliminate androgenic side effects due to the fact that Testosterone itself possesses an androgenic strength rating of 100 and will still act as an androgen in various tissues throughout the body. 5AR blockers such as Proscar, Finasteride, or Dutasteride will not work for anabolic steroids that do not interact with the 5AR enzyme and therefore cannot convert into DHT or any other form of the more potent androgen. These types of anabolic steroids include anabolic steroids that are already DHT-derivatives (and therefore already are existing forms of DHT) such as Anavar, Primobolan, Winstrol, Anadrol, etc., or 19-nor Progestin compounds such as Trenbolone or Deca-Durabolin.
Estrogenic Side Effects (Water Retention)
Through the conversion of aromatizable androgens into Estrogen (touched upon very briefly above under one of the causes for increased blood pressure), anabolic steroids can increase both extracellular and intracellular water retention in the body. Intracellular water, for example, is stored within cells such as the muscle cells that can provide a volumizing and filling effect for the muscles. Extracellular water is located in the circulatory system where, as mentioned above, can cause blood pressure increases[17]. Extracellular water retention also include peripheral water retention underneath the skin (subcutaneous) and can present cosmetic issues for users sensitive to this effect, which would often result in a puffy, soft, bloated look to the physique. A bloated looking face colloquially known as “moon face” can also be associated with this.
The water retention caused by increases in Estrogen is the result of Estrogen’s effect on hypothalamic arginine vasopressin (AVP), which is a hormone involved in the control of water flow in and out of the kidneys[18]. Estrogen is known in this manner to control fluid retention in the body in both sexes[19]. It stands to reason that increased AVP levels are correlated with increased Estrogen levels in the body. Anabolic steroids that do not aromatize (such as Trenbolone, Anavar, Winstrol, and many more) with the exception of Anadrol, do not contribute to this effect.
Water retention and bloating can therefore be effectively controlled or eliminated by either the use of an aromatase inhibitor to reduce total blood plasma levels of Estrogen by way of aromatase inhibition, or through the use of non-aromatizable compounds with low doses of Testosterone. Maintaining a very clean low to moderate sodium content diet without any simple sugars or carbohydrates is one of the most effective methods of controlling all types of water retention, as sodium is one of the key electrolytes responsible for the extracellular retention of water.
Increased bloating and water retention presents increased risks for cardiovascular problems as a result of rising blood pressure and increased fluids in the cardiovascular system. Care should be taken to reduce the incidence of water retention.
Growth Stunting In Children and Teenagers
An interesting effect of anabolic steroids is their ability to increase calcium and mineral retention in bones, as well as increased collagen synthesis. What this translates into is, quite simply: stronger bones and the facilitation of linear growth. As a matter of fact, one of the uses of anabolic steroids in medicine is for the treatment of growth-retardant adolescents and teenagers. Conversely, anabolic steroids also play a role in causing the premature fusion/closing of the growth plates in the human skeleton, which results in stunted growth. There is in fact a significant amount of data in existence that demonstrates a large number of teenage athletes whom have utilized anabolic steroids and experienced stunted growth[20]. There is no specific age known at which the growth plates in individuals close, although much evidence indicates that a large portion of humans continue to grow linearly until the age of 24. The general figure given is that most individuals will continue to grow until the age of 21 – 24 and some even longer. This age range is different for females, which will be explained shortly.
The conditions under which anabolic steroids can stunt growth are actually quite specific, but the risk is still high in individuals who utilize anabolic steroids prior to the closing of growth plates. Specifically, Estrogen is known to play a key role in the fusion of growth plates, halting any possible future growth in both males and females[21]. This is the reason as to why females are generally shorter than males, and it is also the explanation as to why females will halt linear growth at an earlier age. It stands to reason that the vast increases of endogenous Estrogen in the female body in comparison to the male body are what are responsible for this effect.
Therefore, it is the use of anabolic steroids that aromatize into estrogen (or anabolic steroids that will act as Estrogens on their own accord) that is responsible for the closing of growth plates in individuals who have not fully grown, resulting in stunted growth. Age is also a major factor as to how an individual will respond to growth stunting from anabolic steroid use. Very young children for example are much more resistant to the effects of Estrogen on growth plates and would require much longer periods of aromatizable anabolic steroid use before growth stunting manifests itself. Various studies have demonstrated that teenage males at an average age of 14 years old that were treated with Testosterone Enanthate at a dose of 500mg administered once every two weeks for half a year exhibited stunted growth to the extent that final height was reduced by 3 inches in comparison to their predicted final height growth if Testosterone had not been administered[22].
Now, before any individuals think to themselves that non-aromatizable anabolic steroid use should not result in stunted growth, think again: non-aromatizable and non-Estrogenic anabolic steroids have also been implicated in the fusion and closing of growth plates resulting in stunted growth as demonstrated by a study in which Anavar (Oxandrolone) was utilized[23]. Therefore, anabolic steroid use of any sort prior to the physical maturation age of approximately 24 years of age is advised against due to the potential for growth stunting.
Male-Specific Steroids Side Effects
Aside from generalized effects that are not gender specific, there also exists side effects that tend to be experienced by male anabolic steroid users in specific.
Gynecomastia (Breast Tissue Development)
Gynecomastia is the development of breast tissue. Anabolic steroids that present a significant amount of Estrogenic activity either through aromatization or as a direct Estrogenic action from the anabolic steroid itself (i.e. Anadrol, for example) presents a high risk of gynecomastia. Heavily Progestogenic anabolic steroids are also responsible for triggering the development of gynecomastia as well, as Estrogen and Progesterone are key hormones in the dynamic of how breast tissue is developed.
However, Estrogen is the primary culprit here in the development of breast tissue where it binds to receptors in breast tissue and initiates the growth processes of ductal epithelial hyperplasia, ductal elongation, and fibroblast proliferation[24]. On the other hand, androgens actually work to inhibit breast tissue growth[25], which serves to explain why Dihydrotestosterone (DHT) is one of the body’s natural and effective anti-Estrogens. The important note to remember about gynecomastia is that it can only form when the appropriate hormones in the proper ratios are present to form the perfect hormonal environment to favor the development gynecomastia.
The severity, intensiveness, rate of growth, and whether or not this condition may actually manifest itself is dependent on the type of anabolic steroids utilized, the dose, duration of use, as well as the number one determining factor: individual sensitivity to this particular side effect. Many individuals will never experience gynecomastia at all no matter how high Estrogen levels in the body rise, while others may suddenly experience breast tissue development at the sudden onset of the most minimal rise in Estrogen levels.
Gynecomastia development will always progress at varying rates through different stages of development. If gynecomastia development is successfully halted at a particular stage of development, it may be successfully reversed. However, beyond a certain point, the only option possible for the removal of gynecomastia is that of surgery. Every individual should take proper caution to ensure that should the early stages of gynecomastia manifest, that it can be halted before it crosses the irreversible stage. The different stages of development are as follows:
1. Pain and sensitivity in the nipple region (known medically as gynecodynea).
2. Swelling and puffiness of the nipple region (known medically as lipomastia). At this point, glandular tissue is not yet developed and the condition can be reversible if halted here.
3. Complete gynecomastia development (full fatty tissue growth, as well as full glandular growth)

Gynecomastia from anabolic steroid usage
The rate at which these conditions progress is dependent on many factors, but progression can be as rapid as a matter of 2 – 3 days and as long as a number of weeks, where gynecomastia may linger at a certain stage for weeks prior to moving to the next stage of development.
Gynecomastia may be considered a frequent or common side effect of anabolic steroid use, but it is important to make it very clear that: it is a completely avoidable side effect. As a matter of fact, gynecomastia is perhaps the most easily avoidable of any anabolic steroids side effects. The use of a SERM (Selective Estrogen Receptor Modulator) such as Nolvadex proves very effective at not only blocking the development of gyno, but also halting it in its tracks. SERMs are compounds that serve to act essentially as ‘fake’ Estrogens and attach to the receptors in breast tissue and block Estrogen from its ability to bind to and activate these receptors. SERMs such as Nolvadex do not serve to reduce total Estrogen levels in the body – they merely block Estrogen’s effects in certain target tissues. In order to reduce total blood plasma levels of Estrogen, the use of an aromatase inhibitor (AI) is necessary, where AIs work to inhibit the enzyme responsible for the conversion of androgens into Estrogen, thereby reducing the cause of rising Estrogen levels at the root cause. A combination of both an AI and a SERM during periods of gynecomastia development is best recommended so as to ‘attack’ the gynecomastia issue from all angles and provide fast effective relief and reversal of the condition.
One additional potential factor in the development of gynecomastia must be mentioned: the issue of Progestins and Progesterone. Progesterone and Progestogenic anabolic steroids and hormones have been known to also play a key role in the development of gynecomastia in the sense that they potentiate the effects of Estrogen on breast tissue growth[26]. Estrogen and Progesterone receptors both exist in breast tissue and it is believed that the activity of the Estrogen receptor exacerbates the sensitivity of the Progesterone receptor (and vice versa, as Progestins can increase the sensitivity of Estrogen receptors). What this means is that anabolic steroids that exhibit a high level of Progestogenic activity, such as Trenbolone and Nandrolone, when binding to and activating the Progesterone receptor on breast tissue, can and will cause the Estrogen receptor to become more sensitive to circulating Estrogen levels and increase the chances of gynecomastia. The result is an environment in which even the lowest Estrogen levels can trigger the development of gynecomastia. The intricate combination of Estrogen, Progesterone, and Prolactin create a complex network by which gynecomastia can become a massive issue. In such cases, a SERM such as Nolvadex will prove successful in treating, blocking, and preventing this effect.
Testicular Atrophy and HPTA Suppression
Every single anabolic steroid exhibits a suppressive effect on the endogenous production of Testosterone by way of the Hypothalamic Pituitary Testicular Axis (HPTA) negative feedback loop. There currently exists no anabolic steroid that is an exception to this rule. The exogenous administration of anabolic steroids will suppress and/or shut down natural endogenous Testosterone production for the duration of its use.

Anabolic Steroid Induced Hypogonadism (ASIH)
Most usually a visible effect of HPTA suppression/shutdown is that of testicular atrophy whereby the testes shrink in size due to a lack of stimulation in the form of gonadotropins (hormones that travel to the testes to signal the Leydig cells to begin the manufacture and secretion of Testosterone) such as Luteinizing Hormone (LH) and Follicle Stimulating Hormone (FSH). If this stimulation is nonexistent for an extended period, the testicles can lose volume and shape, and essentially shrink in size. Testicular atrophy has been found to be one of the most common side effects among anabolic steroid users, found to appear in slightly over 50% of all anabolic steroid users[27] [28]. Roughly half of all anabolic steroid users will also never experience this side effect – once again, individual response. As well, testicular atrophy may be one of the most common anabolic steroids side effects, but it is also known to be the most temporary and very reversible side effect[29]. Various anabolic steroids may present more suppressive shut-down than others, but all anabolic steroids exhibit this effect of HPTA suppression and eventual shutdown as duration of use continues.
Immediately following the end of any anabolic steroid cycle, it is highly advised that the user engage in a proper PCT (Post Cycle Therapy) protocol, which includes the use of Testosterone production stimulating ancillary compounds, such as Nolvadex and/or HCG (Human Chorionic Gonadotropin, a synthetic Luteinizing Hormone) for a typical PCT period of 4 – 6 weeks following the end of a cycle. Failure to do so can result in permanent damage to the HPTA (Hypothalamic Pituitary Testicular Axis) whereby the individual will insufficiently produce proper levels of Testosterone for life, ultimately requiring medical intervention in the form of TRT (Testosterone Replacement Therapy).
Female-Specific Steroids Side Effects
Aside from generalized effects that are not gender specific, there also exists side effects that tend to be experienced by female anabolic steroid users in specific.
Deepening of the Voice (Dysphonia)
Deepening of the voice is a common side effect belonging to a list of anabolic steroids side effects specific to females known as virilization (the development of adult male physical characteristics in a female or a young boy). Technically, these are androgenic effects but they are far more pronounced in females than in males, and deserve their own category.
Androgens affect the larynx as well as the muscles involved in the generation of vocal sounds and development. This is why males in general have deep voices in comparison to females. The development of dysphonia in females as a result of anabolic steroid use occurs slowly in stages almost reminiscent of gynecomastia development in men. In any case, the development of dysphonia is usually characterized by the early onset of the beginnings of a hoarse voice, followed by variations in pitch as well as the typical ‘cracking’ of the voice commonly seen in pubescent young males[30].
The rate at which these changes take place and the degree to which they change is dependent on the anabolic steroid used, doses used, as well as duration of use. Anabolic steroids that possess a very strong androgenic strength rating (such as Testosterone and Trenbolone) will exhibit high tendencies of producing vocal changes in female users, especially when high doses are used and as duration of use becomes longer and longer. This is why it is advised that females avoid strong androgens and to instead opt for the anabolic steroids that are considered mild in androgenic strength. Other proper precautions include cycle lengths that are as short as possible (approximately 4 weeks for females), and sensible doses. All anabolic steroids, despite some being very mild or very strong in terms of androgenic effects, will all generate dysphonia if utilized long enough, at high enough doses.
Upon the first signs of vocal changes, it is advised that female users immediately discontinue the administration of any anabolic steroids. If halted early enough, dysphonia can often be reversed, but when left beyond a certain point, changes can be irreversible.
Clitoral Enlargement (Clitoromegaly)
Male and female sex organs are closely related in many ways and respond the same way to androgenic hormones. Just as Testosterone during male puberty is associated with generating changes in penile size that favor growth of the sex organ, increased androgens in the female body can and will generate growth of the clitoris (which is very closely related to the male penis).
Clitoromegaly can progress from very minor almost unnoticeable growth to excessive enlargement of the clitoris when androgen levels in women remain high enough for long enough periods of time to facilitate this growth. Once again, as with nearly all anabolic steroids side effects, growth and enlargement of the clitoris is very much dose dependent, duration dependent, and compound-type dependent. Just as with the issue of dysphonia (deepening of the voice), weaker androgens are preferred for female use (Anavar, Winstrol, Primobolan, etc.) at sensible doses over the very strong androgens (Testosterone, Tren) that will tend to bring about this side effect far quicker and more severely.
Increased Hair Growth (Hirsutism)
This particular side effect is also experienced by male anabolic steroid users as well, although it is less noticeable and generally not an inconvenient side effect for men, as the majority of males already possess bodily hair growth as a result of natural Testosterone production. In females, anabolic steroids have the potential to cause male hair growth (growth of hair on the face, chest, abdomen, back, legs, etc.). Just as with the other listed side effects, hirsutism is also dependent on the type of anabolic steroid used, the dose, and duration of use.
Menstrual Irregularities
Anabolic steroids due to their hormonal actions will result in menstrual cycle changes in female users. This can result in both frequent menstruation as well as infrequent or no menstruation at all. The cessation of anabolic steroid use most usually always results in the return of normal menstrual cycles and fertility. Recovery can range from a period of weeks to months depending on the length of cycles, dose used, and type of anabolic steroid(s) utilized.
Breast Size Reduction
As mentioned above under the gynecomastia side effect for males, androgens in the human body actually work to inhibit breast tissue growth24, and in females in particular, the use of anabolic steroids has been demonstrated to cause a shrinkage in breast tissue size in female-to-male transgender patients administered Testosterone in long-term duration of use[31]. Unlike various other female-specific androgenic side effects associated with anabolic steroid use, breast size reduction can remain following the termination of anabolic steroid use. This is because in an androgen-rich environment, the development of breast tissue reconstruction is very prominent. Once again, this is a side effect that is highly dependent on the type of anabolic steroid used, the dose, and duration of use.
Medical References:
[1]Use of anabolic steroids and associated health risks among gay men attending London gyms. Bolding G, Sherr L, Elford J. Addiction. 2002 Feb;97(2):195-203.
[2] Hepatic lipase activity influences high density lipoprotein subclass distribution in normotriglyceridemic men: genetic and pharmacological evidence. Grundy S et al. J Lipid Res 1999 40:229-34.
[3] Changes in lipoprotein-lipid levels in normal men following administration of increasing doses of testosterone cypionate. Kouri EM et al. Clin J Sport Med 1996 Jul;6(3):152-7.
[4] Contrasting effects of testosterone and stanozolol on serum lipoprotein levels. JAMA 261:1165-8, 1989.
[5] High-density lipoprotein choilesterol is not decreased if an aromatizable androgen is administered. Friedl K, Hannan C et al. Metabolism 39(1) 1990.
[6] Relationship of cardiac size to maximal oxygen uptake and body size in men and women. Hutchinson PL, Cureton KJ, Outz H, Wilson G. Int J Sports Med. 1991 Aug; 12(4):369-73.
[7] Androgenic anabolic steroids also impair right ventricular function. Kasikcioglu E et al. Int J Cardiol 2008 Feb 11 E Pub.
[9] Adverse effects of anabolic androgenic steroids on the cardiovascular, metabolic and reproductive systems of anabolic substance abusters. Tuomo Karila. Publications of the National Public Health Institute ISBN 951-740-388-2.
[10] Effects of training on left ventricular structure and function. An echocardiographic study. Shapiro CM et al. Br. Heart J 1983; 50:534-39.
[11] Homocysteine induced cardiovascular events: a consequence of long term anabolic-androgenic steroid (AAS) abuse. M R Graham. F M Grace et al. Br. J Sports Med. 2006;40:544-48.
[12] Enzyme induction by oral testosterone. Johnsen SG, Kampmann JP, Bennet EP, Jorgensen F. 1976 Clin Pharmacol Ther 20:233-237
[13] Anabolic-androgenic steroids and liver injury. M Sanchez-Osorio et al. Liver International ISSN 1478-3223 p. 278-82.
[14] Mechanisms and sites of action of ursodeoxycholic acid in cholestasis. Beuers U. Nat Clin Pract Gastroenterol Hepatol 2006; 3:318-28.
[15] Effect of testosterone and anabolic steroids on the size of sebaceous glands in power athletes. Kiraly CL et al. Am J Dermatopathol, 1987 Dec, 9:6, 515-9.
[16] RU 58841, a new specific topical antiandrogen: a candidate of choice for the treatment of acne, androgenic alopecia, and hirsutism. Battmann T. et al. J Steroid Biochem Mol Biol. 1994 Jan;48(1):55-60.
[18] Effect of ovarian steroids on vasopressin secretion. Forsling, M. L., P. Stromberg, and M. Akerlund. J endocrinol. 95: 147-151, 1982.
[19] Sex hormone effects on body fluid regulation. Stachenfeld NS. Exerc Sports Sci Rev. 2008 Jul;36(3):152-9.
[20] Hormonal doping and androgenization of athletes: a secret program of the German Democratic Republic government. Franke WW, Berendonk B. Clin Endocrinol. 2001 Jun 10;178(1-2):215-20.
[21] Effects of estrogen on growth plate senescence and epiphyseal function. M Weise, S De-Levi et al. Proc Natl Acad Sci June 5, 2001 pp. 6871-6876.
[22] The results of short-term (6 months) high-dose testosterone treatment on bone age and adult height in boys of excessively tall stature. Bramswig JH, von Lengerke HJ et al. Eur J Pediatr. 1988 Nov;148(2):104-6.
[23] Oxandrolone in constitutional delay of growth: analysis of the growth patterns up to final stature. Bassi F, Neri AS, Gheri RG, Cheli D, Serio M. J Endocrinol Invest. 1993 Feb;16(2):133-7.
[24] Estrogen regulation of mammary gland development and breast cancer: amphiregulin takes center stage. Heather L LaMarca and Jeffrey M Rosen. Breast Cancer Res. 2007; 9(4):304.
[25] Androgens and mammary growth and neoplasia. Dimitrakakis C, Zhou J, Bondy CA. Fertil Steril. 2002 Apr;77 Suppl 4:526-33.
[26] Roles of estrogen and progesterone in normal mammary gland development insights from progesterone receptor null mutant mice and in situlocalization of receptor. Shyamala G. Trends Endocrinol Metab. 1997 Jan-Feb;8(1):34-9.
[27] Use of anabolic steroids and associated health risks among gay men attending London gyms. Bolding G, Sherr L, Elford J. Addiction. 2002 Feb;97(2):195-203.
[28] Indications of prevalence, practice and effects of anabolic steroid use in Great Britain. Korkia P, Stimson GV. Int J Sports Med. 1997 Oct;18(7):557-62.
[29] A combined regimen of cyproterone acetate and testosterone enanthate as a potentially highly effective male contraceptive. C Meriggola et al. J Clin Endocrinol Metab 81(8) 3018-23, 1996.