


Oral Steroids Introduction
The topic of oral steroids is perhaps the most popular topic among especially newcomers and prospective anabolic steroid users. There exists no greater attraction to those looking into using anabolic steroids for the first time than the attraction of the convenience of anabolic steroids in a very convenient easy to swallow pill or capsule format. Prior to describing the basics of what oral anabolic steroids are, how they work, what they do, and how they differ from other formats (such as injectables), it is very important to first clarify several misconceptions about oral anabolic steroids that seems to propagate the uneducated general public. They are the following:
– Misconception #1: Oral steroids are safer than injectables.
– Misconception #2: Oral steroids are less effective/strong or more effective/strong than injectables.
– Misconception #3: Oral steroids are easier to obtain.
– Misconception #4: Oral steroids are cheaper.
Misconception #1: Oral steroids are safer than injectables.
This is perhaps the largest misconception among oral anabolic steroids, and is perhaps the second overall largest misconception in regards to anabolic steroids in general (with the first largest misconception/myth/rumor being that anabolic steroids will generate massive muscles without any hard work, training, or diet). The real truth is that both injectable and oral steroids both contain various risky compounds in each category. There exist oral steroids that present a higher risk of various dangers to the body, while there are also injectable steroids that present higher risks as well. When it comes down to it, oral steroids are both harsher on the body’s subsystems than the majority of injectables, and although there are one or two ‘milder’ and ‘safer’ oral steroids, the majority of them present issues of hepatotoxicity (liver toxicity) and negative cholesterol alterations that are far more impacting than most injectables. This is not a problem present with the majority of injectables with the exception of a select one or two, as the majority of injectable compounds are well tolerated by the body. The specific details in regards to why this is the case will be explained shortly in this article.
Misconception #2: Oral steroids are less effective/strong or more effective/strong than injectables.
Oral steroids are not stronger than injectable steroids, nor are they weaker. The anabolic strength rating (the determined measurement of how effective an anabolic steroid is in terms of the promotion of muscle growth) of various oral anabolic steroids does indeed match or surpass the anabolic strength rating of many injectable compounds, while several oral anabolic steroids fall short when compared to injectable compounds as well.
Misconception #3: Oral steroids are easier to obtain.
Simply put, this is not true. There exists highly popular anabolic steroids in both categories that are very easy to obtain, but it just so happens to be that the most popular anabolic steroid of all time is an oral steroid (Dianabol, AKA Methandrostenolone). Aside from this, the next two most popular anabolic steroids of all time are both injectables: Nandrolone (Deca Durabolin) and Winstrol (Stanozolol). All anabolic steroid sources and vendors should carry all types of oral steroids and injectable steroids in equal amounts available for purchase.
Misconception #4: Oral steroids are cheaper.
This is also not true. Within both categories (oral and injectable), there are both more expensive compounds as well as less expensive compounds, all related to factors such as popularity of the compound, ease of manufacture, ease of access, and so on and so forth. The overall price of an anabolic steroid cycle will also normally end up being the same in general, as anabolic steroid cycles should ideally be pre-planned and all costs and dosages calculated prior to purchase. At the end of the day, the overall cost of the amount of oral steroids to run in any given cycle is often almost the same price as any other injectable compound, with the exception of various more expensive compounds as mentioned prior. However, when compared to many injectable compounds, simple cycles, for example, of an injectable format of Testosterone ends up being far more cost effective than oral steroid cycles.
Oral Steroids: What They Are, How They Work
It is absolutely imperative to understand that the only three conventionally and commercially available oral steroids that are bioavailable orally without the need for chemical modification are Andriol, Primobolan, and Proviron. Other than these three, all oral anabolic steroids must have previously undergone a specific modification in order to allow oral bioavailability. When Testosterone (or any other anabolic steroid) is ingested orally, very little of it will enter the bloodstream – too little, in fact, to impart any significant effects on the body. This is because all ingested substances that are swallowed and processed through the gastrointestinal (GI) tract must always undergo what is known as a first pass through the liver prior to finally entering the bloodstream. Unfortunately, nearly all anabolic steroids are very easily metabolized and broken down by the liver, leaving a very miniscule percentage that actually survives this liver metabolism.
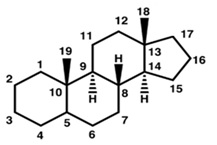
Figure 1: A basic image of the basic steroid structure indicating the numbered carbon positions
It was then discovered at one point, that by modifying the chemical structure by adding a methyl group (also known as an alkyl group) to the 17th carbon on the steroid structure (also known as carbon 17-alpha), it would allow the anabolic steroid to become more resistant to hepatic metabolism. This chemical bonding of a methyl group onto the 17th carbon is known as C17-alpha alkylation. As previously mentioned, when an anabolic steroid becomes C17-alpha alkylated, it allows an anabolic steroid to become orally active and bioavailable – without it, the anabolic steroid would not survive liver metabolism. However, the negative downside in this case is that of increased hepatotoxicity (increased liver toxicity). C17-alpha alkylation allows an anabolic steroid to become more resistant to hepatic breakdown, and any compound that is further resistant to hepatic breakdown will always have greater hepatotoxicity associated with it for various reasons.

Figure 2: A methyl group, which is a central carbon atom bound to three hydrogen atoms, with one available opening to bond to the steroid molecule
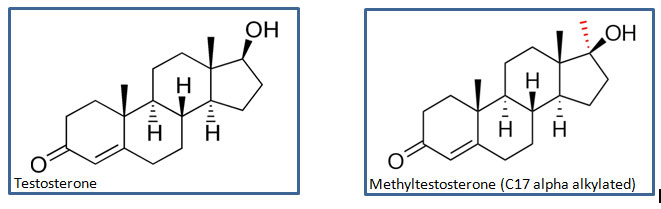
Indicated above is the difference between Testosterone without methylation (C17-alpha alkylation) and beside it is an image of Methyltestosterone, which is of course, C17-alpha alkylated Testosterone in order to allow Testosterone to become bioavailable orally and survive liver metabolism. The added methyl group is then indicated by the broken up red lines forming an arrow-like point at the 17th carbon position, indicating that the methyl group is resting behind the visible orientation of the molecule shown (a solid line forming an arrow-like point indicates the methyl group is situated in front of the visible orientation of the molecule).
The C17-alpha alkylation of an anabolic steroid therefore places select limitations on how it can be utilized, how long it can be used, and the dosing schemes of an oral steroid. These limitations surround its hepatotoxic effects on the liver, as well as its deleterious effects on cholesterol levels in the body.
The following is a list of the most popular and most common C17-alpha alkylated oral steroids (in order of popularity):
– Dianabol (Methandrostenolone)
– Winstrol (Stanozolol)
– Anavar (Oxandrolone)
– Anadrol (Oxymetholone)
– Turinabol (Chlorodehydromethyltestosterone)

Advertisement
Oral Steroids and Hepatotoxicity (Liver Toxicity)
It is important to understand that not all C17-alpha alkylated oral steroids exhibit the same amount or level of hepatotoxicity. There are various oral steroids that are known to be significantly hepatotoxic (such as Anadrol, AKA Oxymetholone), while there are oral steroids that are known as being fairly mild in terms of their hepatotoxicity (such as Anavar, AKA Oxandrolone). The determining factor in what causes one oral steroid to exhibit more liver toxicity over another is a question of debate and is not known with 100% certainty, but it is understood that various anabolic steroids are naturally more resistant to hepatic metabolism before they undergo the methylation, and following the methylation, their hepatic metabolism resistance is furthered to even greater degrees. A perfect example of this is the anabolic steroid Trenbolone, which is an injectable anabolic steroid that does not possess C17-alpha alkylation, and on its own does not exhibit any notable hepatotoxicity. It is, however, known to be quite resistant to hepatic metabolism on its own right. Following C17-alpha alkylation of it, creating Methyltrienolone, it then exhibits one of the most extreme degrees of liver toxicity ever reported – so much so that it is in fact for the most part un-useable. Its resistance to hepatic metabolism is so great that it has been labeled as being “exceedingly liver toxic”, where studies conducted on it in 1966 determined it to be the most hepatotoxic oral steroid ever recorded[1].
All C17- alpha alkylated oral steroids have displayed at least some level of hepatotoxicity in studies, and what is very important to make note of is the fact that in many of these studies, doses utilized were medical therapeutic prescription doses that are generally doses of oral steroids that are far lower than those the doses of oral steroids required for performance and physique enhancement. A perfect example to examine is Dianabol, as it is without a doubt the most popular oral anabolic steroid. Studies have demonstrated that Dianabol doses of 15mg per day or more displayed elevated bromosulphalein levels (an indication of increased hepatic strain), and at doses of 10mg or less per day displayed minimal hepatic strain[2]. This would indicate that Dianabol’s hepatotoxicity will always increase in relation to the dose used, and is the case for all oral steroids that happen to be C17-alpha alkylated. In terms of how the doses in the aforementioned study relate to real world bodybuilding doses, one could easily see how liver toxicity could potentially become an issue seeing as though the minimum beginner dose for bodybuilding purposes for something like Dianabol is no less than 25mg per day on average.
The most common form of hepatotoxicity as a result of excessive oral anabolic steroid use is known as a condition called Cholestasis[3]. This is a condition whereby bile flow in the liver becomes either completely halted or at the very least disrupted. This can result from either a physical blockage, or a chemical one (as is the case with anabolic steroid induced cholestasis of the liver). What occurs here is that the blockage or chemical impairment results in a buildup of bile salts and bilirubin in the liver and bloodstream. In large enough quantities, this build-up can become toxic to the hepatic cells of the liver and kill them. The severity of this condition can range from very minor and discomforting to life-threatening. Minor cases are recoverable in a matter of weeks while more severe cases may require months or more of recovery time.
The excessive abuse of oral steroid doses as well as oral steroid cycle lengths can potentially cause very serious liver problems that can (and have in the past) become life-threatening. Many individuals have developed liver cysts, hepatocellular necrotic lesions (liver cell death and scarring of liver tissue), and in rare cases, hepatic angioscarcomas and hepatocellular carcinoma (liver cancers). These have been found in a couple of bodybuilders following high-dose regimens of oral anabolic steroids[4], as well as one well documented death[5].
Oral steroids and Negative Cholesterol Changes
It is a well-known and very well documented fact that anabolic steroids can and do exhibit negative cholesterol changes on the body, and various anabolic steroids exhibit this to a lesser extent, and some to a greater extent, while some anabolic steroids have displayed the ability to alter cholesterol levels in a positive manner (though this is very rare). In the case of oral steroids, this negative impact on cholesterol levels is in fact the worst of all types of anabolic steroids. These changes involve the reduction of HDL (the good cholesterol) and increases of LDL (the bad cholesterol). The result of such changes involves an increased risk of arteriosclerosis, and the degree to which these changes occur for the worse are usually dose-dependent (with higher doses increasing the negative changes and the risks). Other factors that affect these negative cholesterol changes are: duration of use, and route of administration. This is where oral anabolic steroids hold a negative reputation for exhibiting a far worse negative impact on cholesterol in comparison to injectable anabolic steroids. This is because the liver serves to function as the cholesterol processing center for the human body, and the increased hepatotoxicity associated with anabolic steroids will result in even worse negative cholesterol changes. Anabolic steroids have a profound effect on increasing an enzyme in the liver known as hepatic lipase, which is the enzyme that actively metabolizes and breaks down the ‘good’ HDL cholesterol[6]. This results in less HDL cholesterol in circulation in the body during anabolic steroid use.
In order to obtain a proper ‘big picture’ and a proper representation of what is happening, the difference between the effect on cholesterol changes between injectable steroids and oral steroids must be compared. First, injectable steroids and their impacts on cholesterol levels will be examined. Testosterone Cypionate, an injectable non alkylated anabolic steroid was administered in studies at doses of 300mg weekly, which exhibited a 21% reduction in cholesterol levels[7], and an increase to 600mg weekly did not impart any additional reductions in HDL. This data suggests that the impact of cholesterol alterations by injectable Testosterone is not extremely prominent, and that the ceiling for how much of a negative change in HDL will occur seems to be very low. Oral steroids, such as Winstrol (Stanozolol), which is an anabolic steroid commonly known to be much ‘milder’ than Testosterone does not seem to be so ‘mild’ in the area of negative cholesterol alteractions. For example, oral Winstrol in one study was administered at an extremely low dose of 6mg daily for 6 weeks, and resulted in an average of 33 – 71% decrease in HDL cholesterol levels accompanied with an increase in the ‘bad’ LDL cholesterol by 29%. The same study administered 200mg of Testosterone Enanthate, which resulted in only a 9% HDL cholesterol reduction accompanied with a 16% decrease in LDL cholesterol[8]. It is very evident that the negative impact on cholesterol by oral steroids is significant enough to warrant concern.
Limitations of Oral Steroids
As a result of the prominent issues of hepatotoxicity and negative cholesterol changes, it would then be a very smart decision (and is in fact advised even among the medical establishment in prescription guidelines for the use of oral steroids) to run oral steroids for periods no greater than 6 – 8 weeks at any given time in a cycle. This is to ensure healthy liver function, and for proper liver recovery following the cycle. Various oral steroids that are known to exhibit more liver toxicity than others are advised to be used in the range of 4 – 6 weeks, while others can be utilized in the range of 6 – 8 weeks and some perhaps slightly longer (10 weeks maximum). Due diligence must always be undertaken when using oral anabolic steroids in terms of proper liver function and liver health.

Advertisement
It is because of the risk of hepatotoxicity that the main function of oral steroids in any cycle is to primarily serve as a supplementary compound to a solid base of injectable compounds or as a supportive kickstarting compound. No oral steroid should ever be run solitarily on its own. Testosterone in some form no lower than a TRT (Testosterone Replacement Therapy) dose should always be run with an oral steroid. Oral steroids will exhibit suppression of endogenous Testosterone production as severely as any other anabolic steroid, even the oral steroids such as Anavar that are regarded as ‘mild’ compounds[9]. Therefore, Testosterone should always be utilized in some form or another in every single cycle so as to maintain normal physiological functions during a period in which exogenous hormones are used that will suppress and/or shut down the body’s HPTA (Hypothalamic Pituitary Testicular Axis) and endogenous Testosterone production. It is imperative that all individuals (especially beginners) must understand the following very important guideline where anabolic steroid use is concerned:
Absolutely no cycle should ever consist of only oral anabolic steroids under any circumstances.
The decision to run a cycle consisting of only a single anabolic steroid and no injectable compounds is most usually the very first decision of any beginner or prospective individual looking to begin anabolic steroid use. This is usually the result of a fear of needles, but this must be overcome, and once overcome it becomes much easier afterwards. Oral anabolic steroids are not designed to be run solitarily (on their own), and instead serve to act as supplementary compounds to a solid base cycle that should always include injectable compounds, of which an essentially required injectable being Testosterone (for every single cycle). Injectable compounds are the base compounds of any cycle.
For individuals insistent and adamant on engaging in an oral-only cycle, a few examples will be provided very shortly, towards the end of this article.
Kickstarting: ‘Kickstarting’ is a practice that should be used once a beginner has obtained a fair amount of cycle experience to the point where oral anabolic steroids are now stacked with other compounds. This is a technique whereby the user will include an oral anabolic steroid in a cycle for the first several weeks (this is usually done in tandem with a long-estered injectable anabolic steroid due to the longer kick-in period). Because the kick-in period for most injectables (especially long esters) is a matter of a few weeks into a cycle, one usually will not experience the positive effects until such time. The oral anabolic steroid utilized during these first few weeks will enable the user to experience the positive anabolic effects of the oral while the effects of the injectable compound slowly increase. By the time the oral compound is discontinued (or nearing the end of its use), the injectable compound’s anabolic effects are in full swing and a near seamless transition is made. Dianabol is one such anabolic steroid that is commonly utilized to this effect as a kickstarting compound due to its considerable anabolic strength.
Examples of Oral Steroid Cycles
As supplementary components or a kickstart to a base of injectable compounds:
Oral Steroid Cycle Example #1
Weeks 1 – 12:
– Testosterone Enanthate at 300 – 500mg/week
– Nandrolone Decanoate (AKA Deca) at 400mg/week
Weeks 1 – 4:
– Dianabol at 25mg/day
Oral Steroid Cycle Example #2
Weeks 1-12:
– Testosterone Enanthate at 100mg/week
– Nandrolone Decanoate (Deca Durabolin) at 400mg/week
Weeks 1-6:
– Anadrol at 50mg/day
Oral Steroid Cycle Example #3 (high-dose short-term advanced level cycle of 4 weeks)
Weeks 1 – 4:
– Testosterone Propionate at 150mg daily (1,050mg/week)
– Trenbolone Acetate at 150mg daily (1,050mg/week)
– Anavar at 100mg/day
Examples of Oral- Only Cycles
As previously stated, the idea of running a cycle that consists of only oral steroids is, simply put, a bad idea. Without any form of exogenous Testosterone, the body will be incapable of maintaining its normal physiological functions that are normally governed by Testosterone. Other anabolic steroid analogues and derivatives such as oral steroids might perhaps be several times as anabolic as Testosterone, but those are all the benefits most of these compounds possess. For example, Dianabol is a very strong oral steroid with fairly low androgenic effects and very strong anabolic effects – however, it is not a proper androgen for normal bodily function. ‘Normal bodily function’ refers to far more than functions such as libido or other superficial functions that are often over-focused upon by many individuals. The human body and endocrine system are not as simplified as many individuals make it out to be when trivializing an oral steroid only cycle.
Testosterone is vital for proper libido function, it is a regulator of cognitive and physical energy, it regulates the population of thromboxane A2 receptors on megakaryocytes and platelets, and hence platelet aggregation in humans, and it is essential for proper mental and psychological function, and a plethora of other essential functions – so many in fact that a completely separate article could be composed on such a subject and discussed to no end. Because a particular oral steroid is ‘better’ than Testosterone in one or two areas (anabolic tissue increases) and that it might be more convenient to administer, does not mean that it is better than it in every single aspect and function. Many anabolic steroids do nothing in many of those physiological functions that Testosterone is responsible for regulating and governing. Many other anabolic steroid analogues can also serve to in fact mitigate those functions.
The importance of Testosterone notwithstanding, oral-only cycles are extremely limited in the manner by which they can be run. They must be halted earlier than a normal cycle due to the issues of hepatotoxicity, and only one compound at any one given time can be run. The compounding of two or more oral anabolic steroids is a surefire way of dooming the liver to a highly toxic and very unhealthy environment. No more than one oral steroid should be stacked at any one given time, even within properly structured anabolic steroid cycles. Because of the limitations in oral-only cycles, no individual can ever possibly expect the proper physique changes and gains that could be accomplished with a properly structured anabolic steroid cycle. Instead, the potential for gains are limited and/or cut short, or gains are often lost very shortly afterwards.
With that having been established, the following are some examples of oral-only cycles:
Oral-only Steroid Cycle Example #1
Weeks 1 – 8:
– Andriol (non-C17AA oral Testosterone) at 300mg/day
– Anavar at 75mg/day
Oral-only Steroid Cycle Example #2
Weeks 1 – 8:
– Dianabol (Methandrostenolone) at 50mg/day
Oral-only Steroid Cycle Example #3
Weeks 1 – 6:
– Anadrol (Oxymetholone) at 50mg/day
Oral-only Steroid Cycle Example #4
Weeks 1 – 8:
– Winstrol (Stanozolol) at 100mg/day
Medical References:
[1] Liver toxicity of a new anabolic agent: methyltrienolone (17-alpha-methyl-4,9,11-estratriene-17 beta-ol-3-one). Kruskemper, Noell. Steroids. 1966 Jul;8(1 ):13-24.
[2] Anabolic steroids in clinical medicine. Liddle GW, Burke Jr. H A Helvetica Medica Acta, 5/6 1960:504-13.
[3] Anabolic-androgenic steroids and liver injury. M Sanchez-Osorio et al. Liver International ISSN 1478-3223 p. 278-82.
[4] Hepatocellular carcinoma associated with recreational anabolic steroid use. Gorayski P, Thompson CH, Subhash HS, Thomas AC. Br J Sports Med. 2008 Jan;42(1):74-5; discussion 75.
[6] Hepatic lipase activity influences high density lipoprotein subclass distribution in normotriglyceridemic men: genetic and pharmacological evidence. Grundy S et al. J Lipid Res 1999 40:229-34.
[7] Changes in lipoprotein-lipid levels in normal men following administration of increasing doses of testosterone cypionate. Kouri EM et al. Clin J Sport Med 1996 Jul;6(3):152-7.
[8] Contrasting effects of testosterone and stanozolol on serum lipoprotein levels. JAMA 261:1165-8, 1989.
[9] Short-Term Oxandrolone Administration Stimulates Net Muscle Protein Synthesis in Young Men. Melinda Sheffield-Moore, Randall J. Urban, Steven E. Wolf, J. Jiang, Don H. Catlin, David N. Herndon, Robert R. Wolfe and Arny A. Ferrando. Sheffield-Moore et al. Journal of Clinical Endocrinology & Metabolism. August 1, 1999; 84 (8): 2705